
September 24, 2024, Fluoride Action Network announces, “We Won!” In his 9:53 p.m. email, executive director Stuart Cooper writes, “…the United States District Court of the Northern District of California has just ruled on behalf of the Fluoride Action Network and the plaintiffs in our precedent-setting court case.” Cooper shared the decision in a press release late Wednesday. Below is an excerpt from the introduction of the ruling:
“The issue before this Court is whether the Plaintiffs have established by a preponderance of the evidence that the fluoridation of drinking water at levels typical in the United States poses an unreasonable risk of injury to health of the public within the meaning of Amended TSCA. For the reasons set forth below, the Court so finds. Specifically, the Court finds that fluoridation of water at 0.7 milligrams per liter (“mg/L”) – the level presently considered “optimal” in the United States – poses an unreasonable risk of reduced IQ in children..the Court finds there is an unreasonable risk of such injury, a risk sufficient to require the EPA to engage with a regulatory response…One thing the EPA cannot do, however, in the face of this Court’s finding, is to ignore that risk.”
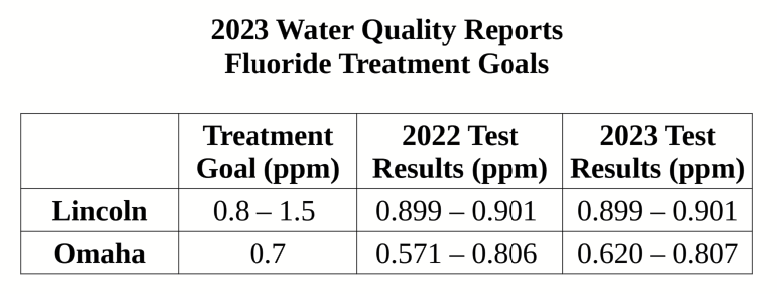
Locally, Nebraska DHHS held a hearing on September 18 to take comments on revisions to the 1983 Title 179 Chapter 1 regulation covering community water fluoridation. Items of note in the revision:
- The revision would lower the fluoridation dosing level to the 2015 USPHS/CDC recommendation of 0.7 mg/L.
- The revision would allow an operational range of ±0.2 mg/L
This revision would allow a treatment level as high as 0.9 mg/L, which could effectively mean no change for Lincoln. A 2015 AWWA report indicates that a ±0.1 mg/L is achievable for nine of 12 months. Given the risk of harms presented in the court ruling, page 5, “a 1-point drop in IQ of a child is to be expected for each 0.28 mg/L of fluoride in a pregnant mother’s urine.” The 2015 USPHS recommendation discusses the quick response of water systems to the 2011 draft. Within six months, by summer 2011, 68% of the water systems population adjusting fluoride at ≥1.0 mg/L was at 0.7 mg/L.
occurring fluoride
Nebraska DHHS Hearing
About thirty people attended the September 18 DHHS hearing on revising the 1983 fluoridation regulation. Four of us spoke on the hazards of chemical fluoridation. With my comments and recommendations, which follow, I provided a copy of the following to be included for the record:
- Supporting References Report
- Holistic Dentistry & Nutrition flyer
- Nourishing Traditions cookbook, by Sally Fallon
- Breaking the Spell, by Tom Cowan
- Weston A Price Foundation: Wise Traditions: 11 Principles booklet
- Weston A Price Foundation: Timeless Principles flyer
Fluoride hearing comments to DHHS, 9/18/24
Thank you for beginning the update to this fluoride regulation and a special thank you to the people from DHHS and NDEE who have responded to my records requests over the last year or so. I’ve been on the receiving end of records requests so I understand the additional workload it can place on already overburdened staff.
It’s my curiosity and love for research that lead me here today. I’ve set out several times over the last 30 years to research healing when conventional health providers for me and my family members failed. What I found most often in my research are stories of doctors finding their own healing after conventional healthcare failed them as well. Then there are other doctors, like Tom Cowan, who find their way by questioning and acknowledging what is not working, and by being curious and creative.
I always claimed that Lincoln had great water even when a few visiting family members questioned it. That changed, though, during 2019 when my research into the events of 9/11 also uncovered that fluoride additives are industrial toxic waste. My research intensified when the predicted censorship of doctors teaching about early, effective, outpatient treatments for respiratory illness actually began during the Covid era.
I’m also into policy, procedures and data analysis. It’s been my hobby, my challenge. I’ve researched and written many procedures over the years – even to the extent of asking to work with auditors during development. The irony of that is, in my naivety and some fear for my job, I took no for an answer. During that time my department, myself included, had to respond to a string of several audits. So, I want to reiterate that I appreciate the pressures of the daily work, of trying to do your best in a job with sometimes little guidance, and of watching others do the same job in wildly different ways without definition for what tasks are important and need to be completed.
So my experience brought me to this question in early 2023, how are we managing the basics? Since fluoride was top-of-mind, I chose simply to see how Lincoln and Lancaster County was managing fluoride treatment. This led me to the state regulation and records requests for, among other things, the procedure to review the 1983 version and the documentation to support the regulation.
While they are extremely important, I won’t elaborate on the reasons to regularly review regulations for important topics such as fluoride or the need for closely examining the age, bias and accuracy of source documents supporting a claim. Experience here shows that only a very small number of people find interest at this level. However, I will share just a few of the many stories I’ve found about how “consensus science” and intimidation influences policy and this particular regulation.
In the early 1950’s not long after fluoridation began, doctors like well-respected allergy specialist George Waldbott in Michigan began receiving referrals for difficult to treat conditions. Waldbott writes of his clinical experience with finding fluoride as the cause, “Chronic poisoning from most toxic agents is rarely diagnosed by physicians in its initial stage. Most systemic poisons induce vague, subtle symptoms before the appearance of features characteristic of a particular kind of poisoning.” For this, correctly diagnosing and healing his patients, Dr. Waldbott was marginalized and dedicated the rest of his life to fluoride education.
By 1990, there was a conference to review the National Toxicology Program’s draft fluoride report. The senior toxicologist for the EPA, Dr. William Marcus, questioned areas of the report related to fluoride and cancer risk. Marcus was soon fired. You will see, in my supporting documents, where the CDC’s 2000 Oral Health Report clearly does not accurately reflect the 1993 NRC’s report on the health effects of ingested fluoride related to credible evidence of harms.
There are so many of these stories, of doctors, scientists, and government employees reluctant to speak out for fear of being marginalized or of loosing respect, and of those who did speak out of lost jobs and credentials.
In addition to regular regulation review with current supporting source documentation, if water fluoridation continues, my recommendations include the following:
Recommendations
- Encourage open access to wise, traditional, nutrient-dense diets and health and healing arts and allow choice and informed consent. I’m leaving you with several references on this with supporting documents.
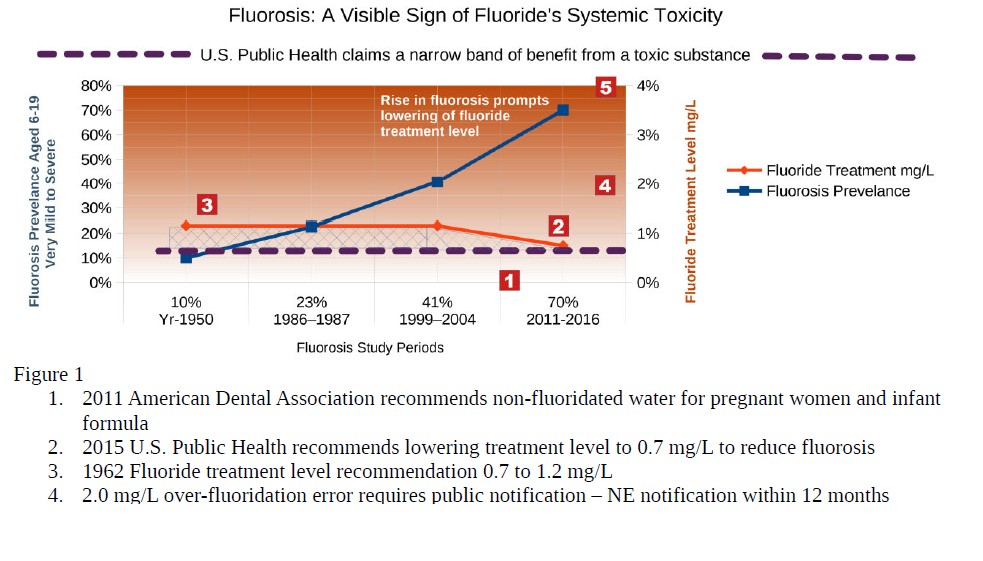
- If fluoridation continues, require warning notification in annual community water reports, and reminders to the dental profession, regarding the 2011 American Dental Association recommendation for pregnant women and infants to avoid fluoridated water.
- Maintain 0.7 mg/L as the maximum fluoride level due to the high risk of bias in studies claiming caries prevention and the vague, subtle symptoms of initial stage chronic poisoning.
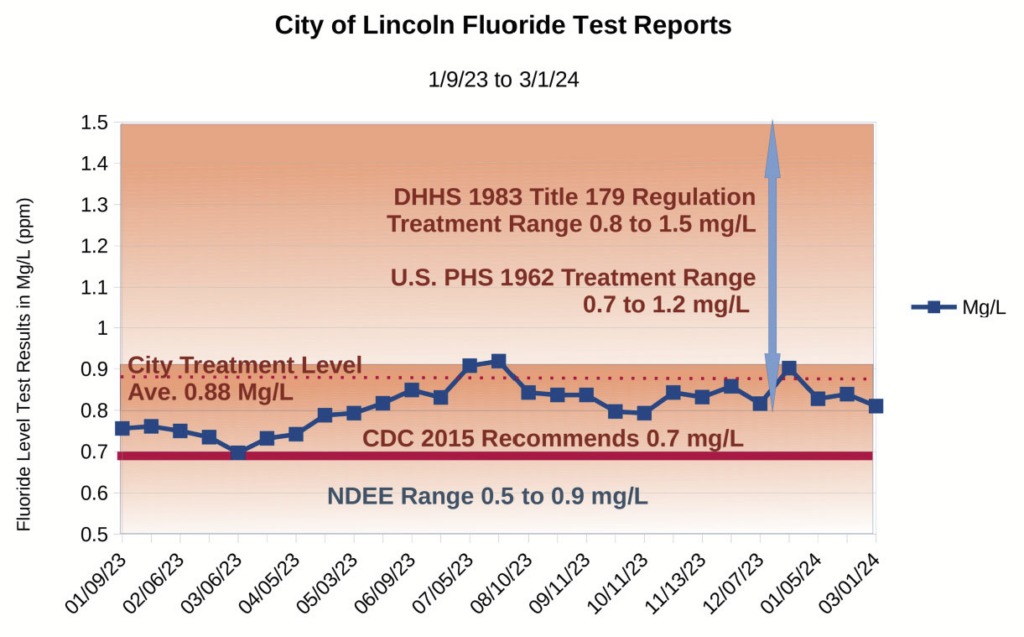
- Lower the operational range to 0.5 to 0.7 mg/L to mitigate harms. As the graph in my supporting document shows, Lincoln test reports and a 2017 AWWA report support the ability to main an operational range within close to ±0.1 mg/L
- Reduce public notification of treatment accidental overdose from 12 months to the number of weeks currently recommended.